
Clinical Nutrition: 危重患者蛋白质摄入量和28天内死亡风险的相关性
2022-06-20 xuyihan MedSci原创

蛋白质是生命活动的物质基础,具有多种生理功能,蛋白质摄入过多过少均不利于健康。因此为了保证身体健康,蛋白质应有适宜的摄入量,保证机体蛋白质“够用而不过多”。
我们知道,在危重疾病的分解代谢阶段,蛋白质是主要的能量底物,而不是正常时期的碳水化合物。身体蛋白质在危重疾病期间响应增加的需求而迅速分解代谢,导致感染并发症增加、恢复时间延长和骨骼肌损失。然而,重症监护病房 (ICU) 中蛋白质摄入的适当剂量和时间仍然存在争议。2016年美国肠外和肠内营养学会/重症监护医学会指南推荐的蛋白质需求量在1.2–2.0g/kg/d,但证据不足。先前的研究表明,早期(第3天前)的低蛋白质(<0.8 g/kg/天)摄入量和后期(第3天后)逐渐增加的分娩与较低的死亡率相关。本研究旨在评估危重患者中蛋白质摄入的不同方式与 28 天死亡率之间的关联。
本项研究是一项多中心、随机对照试验,只要评估积极实施的循证营养指南对危重患者死亡率的影响。纳入的患者是在 ICU 中至少停留7天的患者。应用基于组的轨迹建模来识别该队列中具有相似蛋白质摄入模式的亚组。Cox 比例风险模型用于分析不同轨迹对 28 天死亡率的影响。

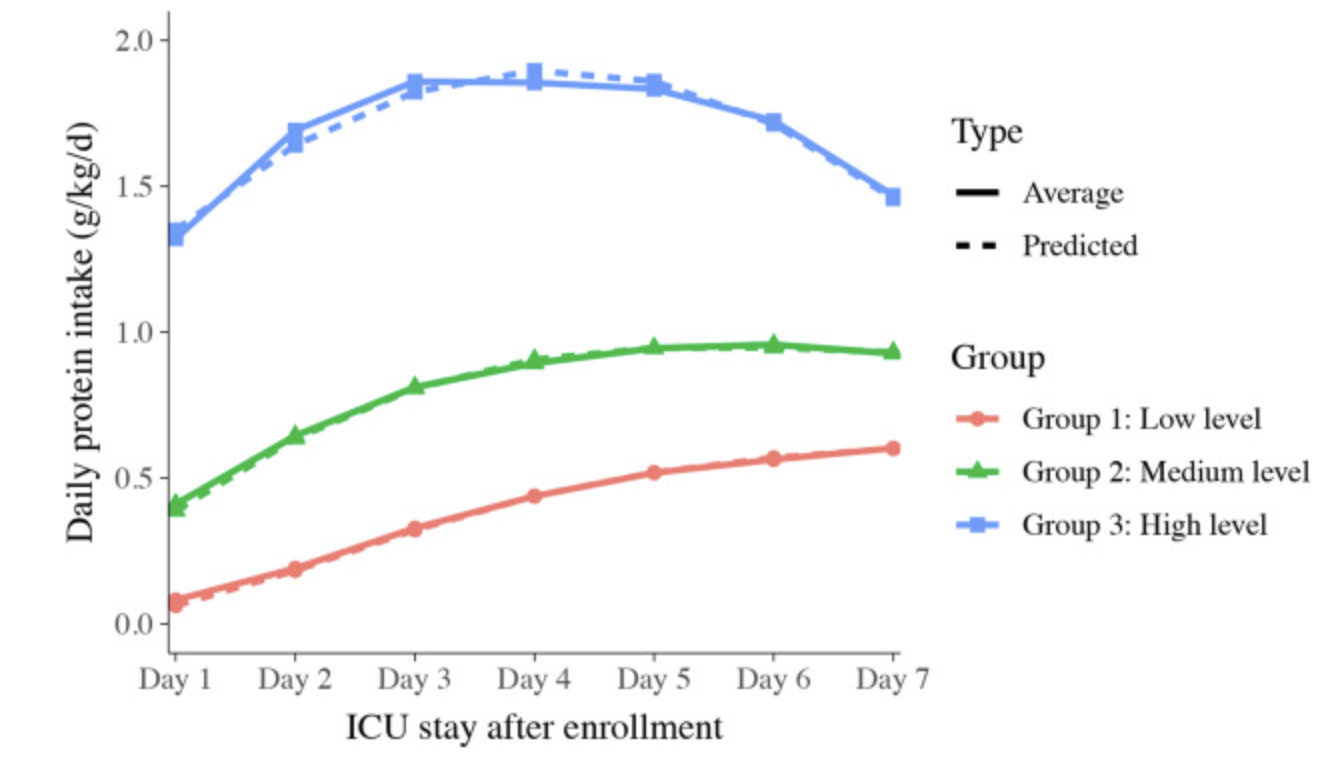
总体而言,2191名患者被纳入分析。确定了蛋白质摄入的明显三种方式,919 名患者分为低水平蛋白质摄入组、1146 名中等水平组和 126 名高水平组。在入组的第一周,从低水平到高水平蛋白质摄入组的平均每日蛋白质摄入量分别为 0.38 ± 0.14、0.8 ± 0.18 和 1.68 ± 0.39 g/kg/d。与中等水平蛋白质摄入组相比,低水平或高水平蛋白质摄入组与 28 天死亡率显着增加相关(风险比 [HR] = 1.348,95% 置信区间 [CI]:1.067–1.704 ; HR = 2.291, 95% CI: 1.533–3.423)。然而,当考虑到能量摄入时,低水平的蛋白质摄入不再与死亡率相关。相比之下,高水平蛋白质摄入的不利影响仍然存在(HR = 2.324, 95% CI: 1.524–3.543, P< 0.001)。
本项研究证实与中等水平的蛋白质摄入相比,危重疾病早期低水平或高水平的蛋白质摄入与 28 天死亡率增加有关。然而,当调整能量摄入时,早期的低水平蛋白质摄入不再与 28 天死亡率增加相关。
原始出处:
JiajiaLin. Et al. Trajectories of protein intake and 28-day mortality in critically ill patients: A secondary analysis of a cluster-randomized controlled trial. Clinical Nutrition.2022.
本网站所有内容来源注明为“梅斯医学”或“MedSci原创”的文字、图片和音视频资料,版权均属于梅斯医学所有。非经授权,任何媒体、网站或个人不得转载,授权转载时须注明来源为“梅斯医学”。其它来源的文章系转载文章,或“梅斯号”自媒体发布的文章,仅系出于传递更多信息之目的,本站仅负责审核内容合规,其内容不代表本站立场,本站不负责内容的准确性和版权。如果存在侵权、或不希望被转载的媒体或个人可与我们联系,我们将立即进行删除处理。
在此留言






#白质#
91
#摄入量#
97
#nutrition#
137
#相关性#
89
#死亡风险#
0
#蛋白质#
87
#clinical#
110