
由于世界范围内的人口老龄化,痴呆症将日益成为个人和社会面临的挑战。由于目前缺乏治疗药物,预防痴呆症已成为一个全球难题。
一些纵向研究发现,特定的疾病(如糖尿病、心房颤动、抑郁症)是导致痴呆症发病率增加的风险条件。事实上,高达90%的60岁以上的成年人有两种或更多的慢性疾病,这种情况被称为多发病。后者与轻度认知障碍和更大的脑部病理负担都密切相关。

由于相似的病理生理机制和/或共同的风险因素,一些疾病往往在同一个人身上聚集,这导致了多病症模式,其特点是慢性疾病系统地聚集在一起。对这种模式的识别提供了有用的临床洞察力,表明特定的多发病模式对痴呆症的发展有潜在的不同影响。
炎症是与特定的多发病模式和痴呆症有关的因素之一。同样,由于脂蛋白E基因变体(APOE ε4)对痴呆症风险的作用是众所周知的,因此有专家假设,特定的多发病模式和APOE ε4等位基因的结合使个人面临更大的痴呆症发展风险。

根据上述假设,来自瑞典卡罗林斯卡学院和斯德哥尔摩大学神经生物学和社会系老龄化研究中心的专家调查了具有不同疾病模式的老年人的痴呆风险,并探索炎症和脂蛋白E(APOE)基因型的作用。相关结果发表在最新的Alzheimer’s&Dementia杂志上。
研究人员纳入瑞典国家老龄化和护理研究(SNAC-K)中共2478名无痴呆症的参与者,他们有两种或更多的慢性疾病(即多发病),根据他们的多发病模式进行分组,并进行跟踪调查,以检测临床痴呆症。通过分层分析测试了C反应蛋白(CRP)和脂蛋白E(APOE)基因型的潜在修饰作用。

按基线多发病率模式划分,每100人年的痴呆症发病率和调整后的危险比
结果显示,与罹患非特异性疾病的参与者相比,患有神经精神、心血管和感觉障碍/癌症等多种疾病的人患痴呆症的危险性分别增加66%、61%和32%(HR=1.66,95%CI:1.13-2.42;1.61,95%CI:1.17-2.29;1.32,95%CI:1.10-1.71)。
当排除了在随访的前6年内发生痴呆的参与者后,得到的结果是一致的。同时,尽管缺乏统计学意义上的相互作用,但在这些模式中,高CRP增加了痴呆风险,而作为APOE ε4携带者则提高了神经精神和心血管多发病的痴呆风险。
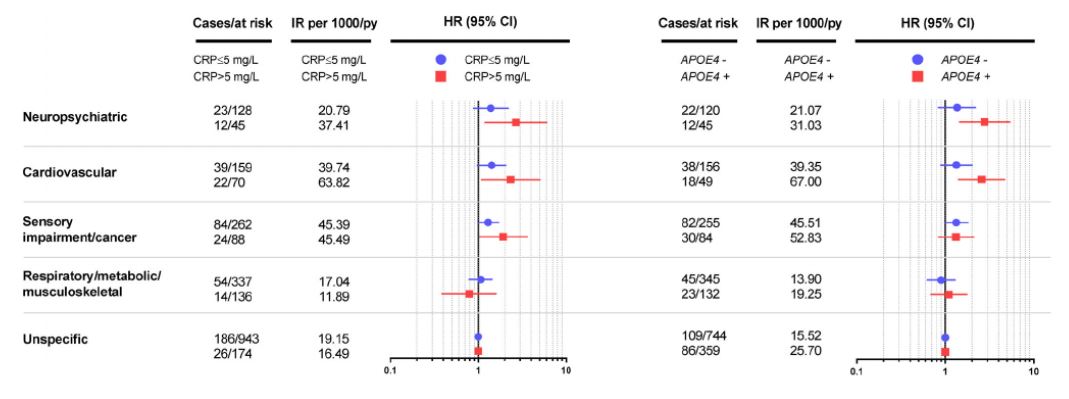
根据血清CRP水平和APOE基因型,按基线多发病率模式划分,每100人年的痴呆症发病率和调整后的危险比
由此可见,有神经精神、心血管和感觉障碍/癌症模式的人患痴呆症和APOE ε4的风险增加,而炎症可能进一步增加风险。识别这样的高危人群可能会对预防痴呆症进行有针对性的干预。
参考文献:
Multimorbidity burden and dementia risk in older adults: The role of inflammation and genetics. https://doi.org/10.1002/alz.12237
本网站所有内容来源注明为“梅斯医学”或“MedSci原创”的文字、图片和音视频资料,版权均属于梅斯医学所有。非经授权,任何媒体、网站或个人不得转载,授权转载时须注明来源为“梅斯医学”。其它来源的文章系转载文章,或“梅斯号”自媒体发布的文章,仅系出于传递更多信息之目的,本站仅负责审核内容合规,其内容不代表本站立场,本站不负责内容的准确性和版权。如果存在侵权、或不希望被转载的媒体或个人可与我们联系,我们将立即进行删除处理。
在此留言






#dementia#
80
#痴呆风险#
64
#遗传因素#
90
老年人痴呆何药可用??
80